In contradistinction to intra-operative mapping, neurophysiological monitoring does not serve to identify the location of critical regions but rather provides real-time information about the integrity of the connections of motor, sensory and auditory systems. As with mapping techniques, monitoring works by initiating an electrical impulse the response of which is interpreted and measured by a trained neurophysiologist. Stimuli and responses are delivered and measured by electrodes placed in the immediate pre-operative period after induction of anesthesia. Motor evoked potentials (MEP) require a stimulus delivered by needle electrodes placed in the scalp or with an electrode strip placed directly on the brain itself (direct cortical MEP) (Figure 1).
Responses are measured from electrodes placed percutaneously in the muscles of the face and limbs. Alternatively, with somatosensory evoked potentials (SSEP) the stimulus is delivered in the extremities and the response is measured from the head. Variables that are measured include the magnitude (amplitude) of the response as well as the time necessary for the electrical message to travel from the stimulus to the terminus (latency). These variables are normally measured in milliamps and milliseconds respectively. Initially baseline measurements are obtained with the patient after induction of anesthesia. Further measurements are taken after final positioning and periodically or continuously during surgery.
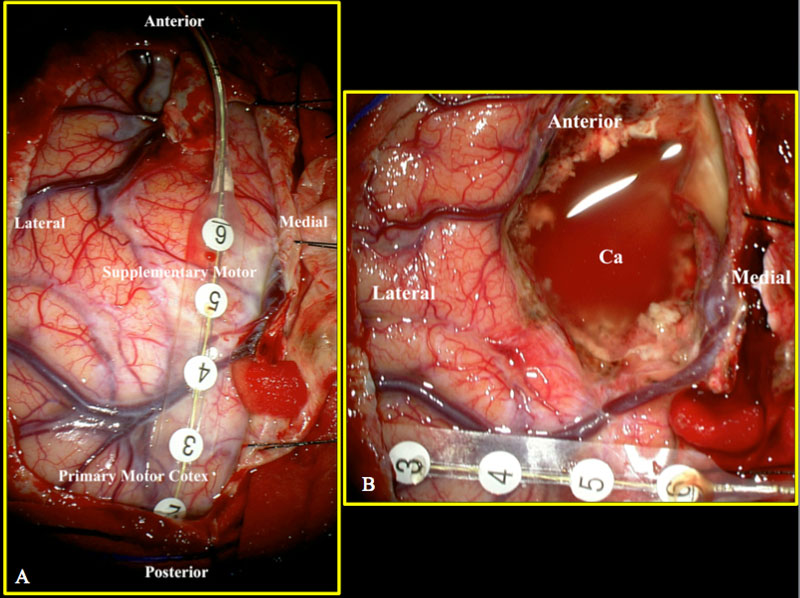
Figure 1 a,b
Intra-operative images obtained during resection of a glioma in the supplementary motor area. Left image (a) demonstrates electrode on brain surface with SSEP phase reversal at electrodes 1 and 2 indicating the junction of the motor and sensory cortex. The strip was then repositioned on the motor cortex allowing for continuous MEP to assure the continuity of descending motor fibers together with subcortical stimulation. The right image (b) was obtained after resection (Ca: tumor cavity).
Maintenance of amplitude and latency infers that the interconnectivity of the motor and sensory systems of the nervous system remains intact. A loss or significant change in these responses suggests that an injury–either reversible or irreversible–to these connections may have been incurred and requires serious consideration. Interpreting alterations in neurophysiological responses requires an experienced neurophysiologist since changes may result from non-critical events such as changes in the depth of anesthesia or the disconnection/malfunction of an electrode. Changes in waveforms may also require a surgeon’s presence of mind in taking necessary steps to prevent a loss of neuronal connectivity. Issues that may be remedied include a change in positioning of the patient’s head and neck, raising the blood pressure, repositioning of brain retractors, or administration of pharmacological agents to dilate blood vessels in the surgical field. Although monitoring serves effectively as an ‘early warning system’ alerting the surgeon of impending injury the hazard of risk, unfortunately, can never be completely eliminated.
Have More Questions about This Condition

New Jersey Brain and Spine Earns #3 National Ranking For Neurosurgical Practices
New Jersey Brain and Spine has once again been recognized among the nation’s elite neurosurgical practices—this time...

Patient Story: Patient Gets Fitness Career Back in Shape Thanks to Dr. Roth
Robin Bray is the owner of FitnessBarre™, a popular local workout studio in Midland Park, New Jersey. The...

NJBS Highlighted for Advanced Tremor Treatment With Hackensack Meridian Health
New Jersey Brain & Spine was recently featured alongside Hackensack Meridian Health, highlighting the impact of...

Patient Story: Ashley’s Recovery After Cervical Disc Herniation
A stroke at birth left Ashley with cerebral palsy and limited mobility on her right side. So when she woke up at 1...

Back on the Competition Track: A Young Athlete’s Recovery After L4–L5 Disc Herniation Surgery
Severe nerve compression brought life to a halt—lumbar microdiscectomy helped him reclaim strength, mobility, and...

Ground-Breaking HiFu Treatment Re-Opens a Door
Innovative non-invasive essential tremor treatment puts car enthusiast back in the driver’s seat Dan lived with...
")
Full Patient Story: Chris’s Recovery After L4–5 Posterior Lumbar Interbody Fusion (PLIF)
How an L4–5 Posterior Lumbar Fusion Gave Chris Feeling in His Leg Again and His Life Back Chris was only in his early...

Back in the Game: Brian’s Recovery After C5–6 Disc Replacement
Neck pain and cervical radiculopathy stole his mobility, his golf swing, and his comfort, an artificial disc...

New Jersey Brain and Spine Launches $2000 Healthcare Scholarship to Support Next Generation of Healthcare Professionals
Investing in the future of healthcare: Annual scholarship open to high school and undergraduate students from or...