Accuracy and conformity of targeting in cranial neurosurgery is achieved through the use of stereotaxis. With this technique, imaging studies are used to create a three dimensional map of the skull and brain or other anatomical structures. This map is co-registered with the patient at the time of treatment and a plan is created allowing for the precise convergence of radiation to exclusively capture the complex 3-dimensional geometry of tumors and AVMs.
The synchronization of a virtual map to the patient may be achieved by either ‘frame based’ or ‘frameless’ systems. In the former, a metal frame is secured to the lightly anaesthetized patient’s head. Each point in space within the boundary of the frame may be ascribed a definable co-ordinate and is targetable. Imaging studies are subsequently obtained thereby creating a unique map of the brain.
After imaging is obtained, neurosurgeons and radiation oncologists work together to delineate the anatomy of pathology. This step in development of the stereotactic plan is called ‘contouring’ and defines the volume of tissue to receive a therapeutic dose of radiation. Physicians make every attempt to create a ‘conformal’ prescription plan where the radiation dose is high within the targeted volume but minimal outside the established perimeter (Figure 1) . Attention to structures that are radiosensitive-the optic nerves, brainstem and cochlea is paramount to avoid radiation induced damage and complications (Figure 2).
Although radiosurgery has its own unique set of limitations, it remains a time tested and vital tool and offers a non-invasive alternative for the treatment of a variety of neurosurgical disorders.
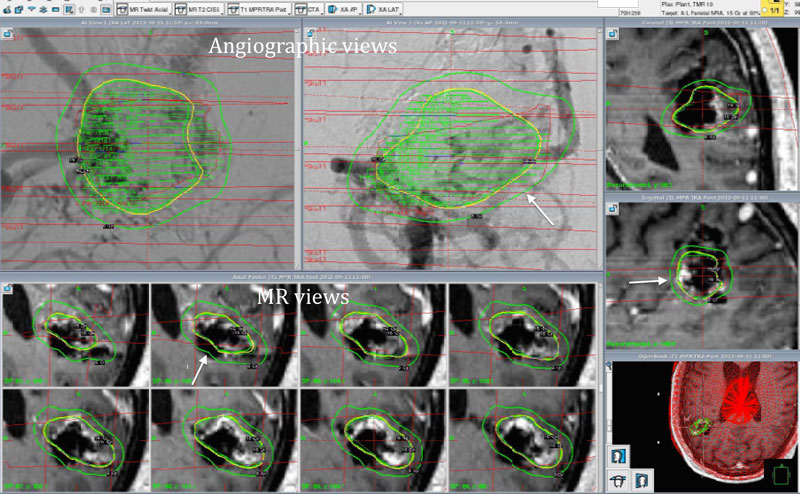
Figure 1
Gamma Knife radiosurgery plan for a patient with a sizable left parietal AVM. Upper left panes demonstrate angiographic anatomy while lower and right sided panes indicate corresponding views by MR. The perimeter of the target (contour) is indicated by the yellow circumference. The green ovoid lines (arrows) indicate the lowest level of radiation received within the boundry (isodose line).
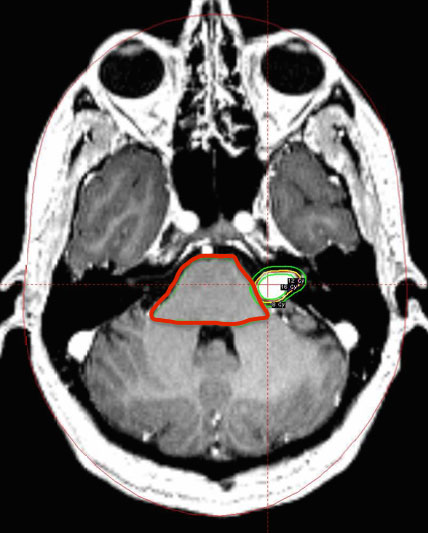
Figure 2
Modified Gamma Knife radiosurgery plan of a left sided vestibular schwannoma. The brainstem has been contoured (red perimeter) to assure radiation dose received is within an acceptable range to avoid post-treatment complications.
Have More Questions about This Condition

Radio host makes airwaves with stroke – and complete recovery
Today, Marisol Vargas is the mother of a vivacious 2½-year-old. But in 2019, she ended up permanently on a daily baby...

Overcoming Essential Tremors: Bob Bosloper’s Story

Reclaiming Your Future: Dana Raleigh’s Story
It Was, Indeed, a Problem Unfortunately, Dana had multiple fractures in her back that she was either born with or...

Flourishing After Parkinson’s Diagnosis: Sandy Deck’s Story
This video highlights the story of Sandy Deck, who was diagnosed with Parkinson’s disease and struggled with…

Discovering New Strength: Patty Petrula’s Story
Patty Petrula was training for her first triathlon when she collapsed at the gym and was rushed to the hospital, where Dr. Daniel Walzman determined she had suffered a ruptured brain aneurysm.
22-year-old Makes Incredible Recovery from Both COVID-19 and Stroke: Danny Dominguez’s Story
As a 22-year-old man, Danny Dominguez isn’t the typical stroke patient. The first time he experienced shortness of breath and headache accompanied by a throbbing sensation in April 2020, he went to a nearby hospital and was sent home with pain medication.
How Neurosurgeon Roy D. Vingan Cured One Patient’s Chronic Back Pain: Stephen Tinney’s Story
Surgery as a Last Resort Many patients with back pain can improve without surgical intervention, and more often than...

Newark Woman Uses Gift Of Hope To Fight Parkinson’s Disease: Susan O’Rourke’s Story
Susan O’Rourke has a gift: she can see hope where others see depression. Now, the president of Newark-based nonprofit Artfront Galleries is harnessing that ability to find a new pathway forward from her battle with Parkinson’s disease.

Surviving Multiple Aneurysms: Michele Blum’s Story
Michele Blum is an actress who lives to be on the stage. But when multiple aneurysms left her in a coma, Michele’s future was far from certain. That’s when Dr. Reza Karimi of New Jersey Brain and Spine entered the stage and found the one path recovery.