What is Brain AVM?
What is a Ruptured Brain Arteriovenous Malformation (AVM)?
A ruptured brain arteriovenous malformation (AVM) is a life-threatening condition in which an abnormally formed tangle of veins and arteries in the brain bursts and causes bleeding into the brain. The bleeding is called a brain hemorrhage and is a serious event that can lead to stroke or brain damage.
Intra-cerebral hemorrhage (ICH) is a general term that defines an accumulation of blood anywhere in the brain. ICH does not necessarily imply the cause of bleeding. Typically, non-traumatic sources include vascular malformations, aneurysms, blood clotting disorders, including those on blood thinners, tumors, and vascular disease resulting from high blood pressure.
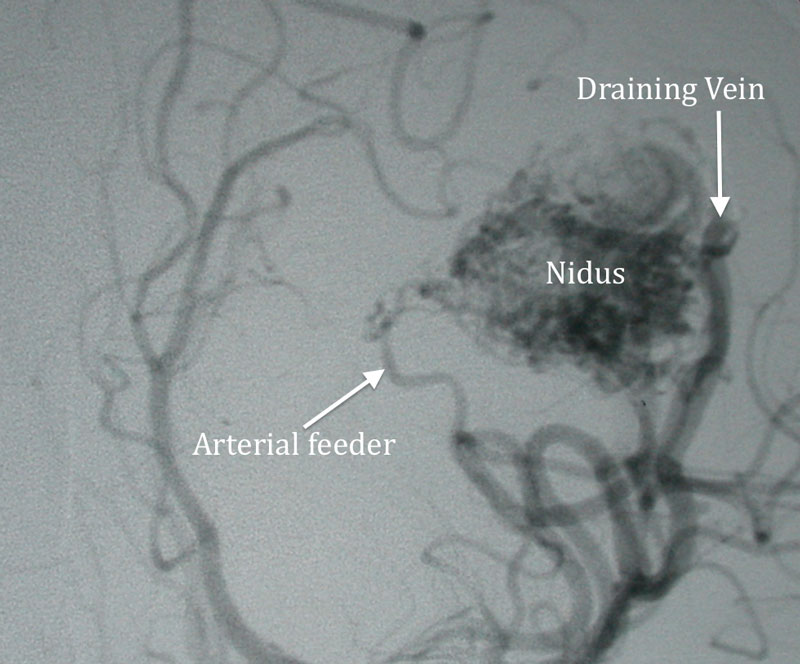
Figure 1
Arterial phase cerebral angiogram demonstrating a large left parietal AVM. Nidus or the center of the AVM is indicated along with feeding arteries and draining vein.
What are the symptoms of a ruptured brain AVM?
Symptoms of an AVM rupture can include:
- Sudden, severe headache
- Loss of consciousness
- Confusion
- Trouble speaking
- Numbness or weakness in the leg, face, or arm
- Paralysis
- Vomiting
- Nausea
Oftentimes, patients with a ruptured brain AVM are taken to the nearest emergency room.
What are the risk factors?
In terms of risk factors, only certain hereditary conditions can increase your risk of having a ruptured brain AVM. These include hereditary hemorrhagic telangiectasia, also known as Osler-Weber-Rendu syndrome.
A family history of an AVM rarely increases your risk. In fact, most types of brain AVMs are not inherited.
What causes a brain AVM?
Typically, arteries carry oxygen-rich blood to the brain and veins carry the oxygen-depleted blood back to the heart. The exchange happens in the smallest blood vessels called the capillaries that act as the “bridge” between the veins and arteries and slow the blood flow. When you have a brain AVM, the capillaries between your veins and arteries are missing and blood flows directly from the arteries to the veins. The pressure can cause one of these vessels to rupture.
In terms of causes for brain AVMs, most doctors find that people are born with the condition and that AVMs develop during fetal development. The condition can become worse over time and may appear at any age.
How is a brain AVM diagnosed?
Diagnosing a brain AVM is difficult before it ruptures. It is critical to locate a ruptured brain AVM quickly. Diagnostic imaging procedures may include the following:
- MRI
- CTA
- MRA
- Cerebral Angiography
Diagnosis of intra-cerebral hemorrhage is established with a head CT scan, and often, the pattern of bleeding suggests the presence of an AVM. Further imaging tests, including CT angiography, MR and MR angiography, support the diagnosis and provide localized anatomical information. A definitive understanding of the anatomy of AVM is obtained from cerebral angiography.
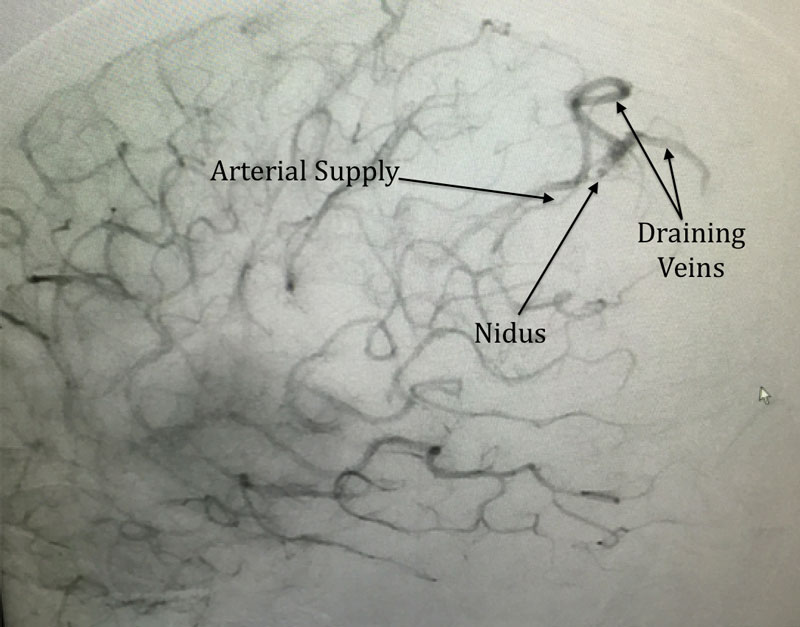
Figure 2
Lateral late arterial phase cerebral angiogram showing a small posterior parietal AVM with indicated arterial supply, nidus and draining vein.
What are the treatment options for a ruptured brain AVM?
An expert team of neurosurgeons can treat a ruptured brain AVM and hemorrhagic stroke with the following methods:
- Open Surgery: This treatment involves removing the abnormal veins and arteries through the opening of the skull to stop the risk of further bleeding.
- Embolization: A minimally invasive catheter procedure involves using glue to seal the abnormal blood vessels.
- Gamma Knife Radiosurgery: This non-invasive procedure involves using radiation on the AVM to reduce the risk of bleeding. At the end of this treatment, patients will have additional imaging done to ensure that the AVM is eliminated.
At New Jersey Brain and Spine, our expert team of neurovascular surgeons is fully trained and equipped in both endovascular embolization and vascular neurosurgery. Therefore, the same surgeon can embolize the AVM, surgically remove it, or treat it with radiation. This unparalleled expertise provides patients with the most optimal treatment options for a complex brain AVM rupture, tailored to each patient’s unique case.
Figure 3
Same patient as above with before and after images superimposed showing embolic material filling the nidus and draining vein.
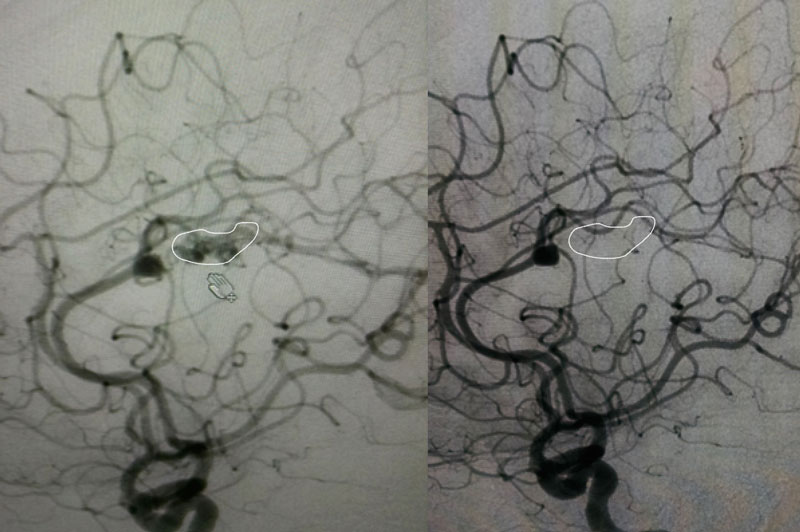
Figure 4
Lateral cerebral angiogram showing small AVM encircled by white line. Right: One year post gamma knife angiogram showing absence of filling (white line indicates estimated location of target) proving obliteration of AVM.
Have More Questions about This Condition

New Jersey Brain and Spine Earns #3 National Ranking For Neurosurgical Practices
New Jersey Brain and Spine has once again been recognized among the nation’s elite neurosurgical practices—this time...

Patient Story: Patient Gets Fitness Career Back in Shape Thanks to Dr. Roth
Robin Bray is the owner of FitnessBarre™, a popular local workout studio in Midland Park, New Jersey. The...

NJBS Highlighted for Advanced Tremor Treatment With Hackensack Meridian Health
New Jersey Brain & Spine was recently featured alongside Hackensack Meridian Health, highlighting the impact of...

Patient Story: Ashley’s Recovery After Cervical Disc Herniation
A stroke at birth left Ashley with cerebral palsy and limited mobility on her right side. So when she woke up at 1...

Back on the Competition Track: A Young Athlete’s Recovery After L4–L5 Disc Herniation Surgery
Severe nerve compression brought life to a halt—lumbar microdiscectomy helped him reclaim strength, mobility, and...

Ground-Breaking HiFu Treatment Re-Opens a Door
Innovative non-invasive essential tremor treatment puts car enthusiast back in the driver’s seat Dan lived with...
")
Full Patient Story: Chris’s Recovery After L4–5 Posterior Lumbar Interbody Fusion (PLIF)
How an L4–5 Posterior Lumbar Fusion Gave Chris Feeling in His Leg Again and His Life Back Chris was only in his early...

Back in the Game: Brian’s Recovery After C5–6 Disc Replacement
Neck pain and cervical radiculopathy stole his mobility, his golf swing, and his comfort, an artificial disc...

New Jersey Brain and Spine Launches $2000 Healthcare Scholarship to Support Next Generation of Healthcare Professionals
Investing in the future of healthcare: Annual scholarship open to high school and undergraduate students from or...